The Body as One — The Scientific Miracle in the Hadith of Wakefulness and Fever
More than fourteen centuries before the emergence of modern physiology, the Prophet Muhammad ﷺ described the internal mechanics of the human body in a single conditional sentence. He did not describe it as a metaphor for Muslim brotherhood alone — he described a literal biological reality: when one organ of the body is injured or ill, the entire body mobilises in response, and its response occurs through wakefulness and fever, in that order. Modern medicine, developed within the last several decades, has confirmed each element of this description with precision that no contemporary of the Prophet ﷺ possessed the scientific framework to articulate.
Al-Nu’man ibn Bashir (RA): “The believers in their mutual love, mercy and compassion are like one body. When one part complains, the rest of the body responds to it with wakefulness and fever.”
Grade: Sahih · Bukhari, Muslim & Ahmad
To understand the depth of this description, we must first examine what science has established about what actually occurs inside a body when one of its organs is injured.
The Body’s Distress Call — Signals from the Injured Organ
Imagine a person in a remote area, far from any medical care, who suffers a severe laceration and blood loss. Before he can seek help, his body has already begun a coordinated emergency response. The injured organ does not remain passive — it immediately broadcasts distress signals across multiple simultaneous axes of the nervous and endocrine systems.
Three distinct channels carry these signals from the wound to the brain’s central command stations.
First — Bleeding and pressure drop: The sudden fall in blood pressure activates baroreceptors and volume mechanoreceptors in the walls of the heart, aorta, and carotid arteries. These sensors transmit nerve impulses directly to the hypothalamic centres of the brain. Simultaneously, pressure sensors in the kidney arteries activate renin secretion, converting angiotensinogen to angiotensin I and then to angiotensin II — which reinforces the hypothalamic alert and causes peripheral vessel contraction to raise blood pressure.Angiotensin II also stimulates the thirst centres and antidiuretic secretion centres, and is among the most potent activators of the adrenal cortex to produce aldosterone. Chemical substances released from the damaged vessel walls simultaneously attract platelets to the wound site and summon phagocytic immune cells to begin their defence.
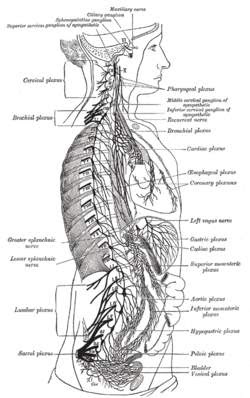
Second — Noradrenaline: Torn nerve endings release noradrenaline into the bloodstream. This hormone travels to the hypothalamic centres, converging with the baroreceptor signals already arriving there.
Third — Pain: Nerve endings at the injury site transmit pain impulses through the spinal cord to the thalamus, then to the sensory cortex and the limbic system, which distributes signals onward to the reticular formation and the hypothalamus.
All three axes converge on the same three nerve centres: the hypothalamus, the higher sensory cortex, and the reticular formation and limbic system. From these centres, the body’s total mobilisation begins.
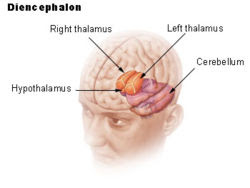
The Hypothalamus — Central Command Station
Upon receiving the distress signals, the hypothalamus activates four major responses in rapid succession.
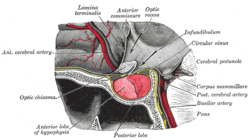
The anterior pituitary is directed to release ACTH (adrenocorticotropic hormone), GH (growth hormone), and TSH (thyroid-stimulating hormone) — each triggering a downstream hormonal cascade that reaches every organ in the body. The posterior pituitary releases ADH (antidiuretic hormone), directing the kidneys to reabsorb maximum water rather than lose it in urine. The sympathetic nervous system receives activating impulses to the cardiac acceleratory centres, respiratory centres, and the adrenal medulla — commanding large-scale secretion of adrenaline and noradrenaline. Finally, in response to pain, the hypothalamus and spinal cord release endorphins and enkephalins.
Endorphins and enkephalins provide an analgesic and reassuring effect estimated at 18 to 30 times greater than that of morphine. This mechanism explains why severely wounded soldiers in combat often feel no pain at the moment of injury — the body suppresses panic to preserve the organism’s capacity to flee or resist.
The reticular formation and limbic system, also alerted at this stage, fulfil a parallel function: maintaining full attention and continuous vigilance in the higher brain centres, and raising the degree of muscle tension and nervous sensitivity throughout the body. Memory centres are simultaneously engaged to direct behaviour toward the crisis based on previous experience — which explains why a body with prior exposure to similar conditions responds more effectively than one encountering it for the first time.
The Hormonal Cascade — Every Organ Activated
The coordinated activation of both the nervous system and the endocrine (hormonal) system in response to physical injury or illness. It is the body’s primary emergency command mechanism, mobilising every organ system simultaneously from a single injury signal.
From the hypothalamus, hormonal and nervous impulses radiate to every organ. The three principal hormones released — cortisol, aldosterone, and adrenaline — cover virtually all vital systems. Cortisol is perhaps the most fundamental: its presence is not merely helpful but essential to life itself in the event of serious illness or injury.
Cortisol supports adrenaline’s action on the heart and blood vessels, stabilises cell membranes, moderates the immune response to prevent excessive immune reactions, and drives the breakdown of proteins, glucose, and fats in muscles and connective tissues — supplying amino acids, fatty acids, and glucose to the liver. In the liver it then promotes the production of new glucose from lactic acid and amino acids (gluconeogenesis) and the manufacture of ketone bodies from fatty acids.
Aldosterone directs the kidneys to retain sodium — which in turn retains water — preserving fluid volume against blood loss. Adrenaline and glucagon break down stored glycogen and fats into glucose, fatty acids, and glycerol; this glucose enters the Krebs cycle to produce ATP molecules in large quantities for the body’s emergency energy requirements. Amino acids are used both for energy production and to build new proteins — antibodies, immune defence cells, and connective tissue molecules necessary for healing.
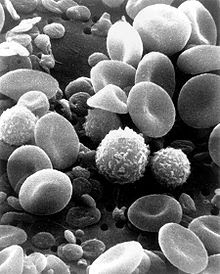
Growth hormone (GH), released by the pituitary under hypothalamic instruction, activates somatomedin in the liver and the tissues of the injured organ, stimulating connective tissue growth and repair. It also activates erythropoietin, which directs the bone marrow to produce new red blood cells to replace those lost to bleeding.
Heart, Blood, and Kidneys — The Supply and Clearance Network
Blood simultaneously transports oxygen, nutrients, hormones, clotting materials, antibodies, and immune cells — all directed toward the affected organ at once. This is the transport medium through which every response described above reaches its destination.
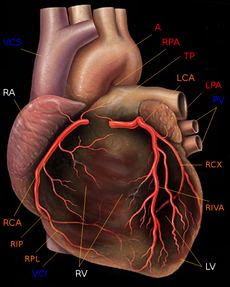
The heart accelerates its rate and strengthens its pumping under both hormonal and nervous stimulation, doubling cardiac output during illness or injury. Peripheral blood vessels contract to redirect blood from less active organs toward the injured area and vital organs. Breathing deepens and accelerates to maximise oxygenation of the increased blood flow.
The kidneys play a dual critical role: they retain water and sodium under the influence of ADH and aldosterone, preserving the body’s fluid reserves; and they continuously excrete the excess potassium released from cells during the catabolic state, preventing the dangerous rise in blood potassium that would cause cardiac arrest if the kidneys failed this function.
The liver increases its metabolic activity, the endocrine glands sustain their hormonal output, muscles contribute their protein reserves, and fat stores are broken down — all redirecting the body’s essential materials toward the single site of injury. The destruction of the body’s own tissues in service of the injured organ continues proportionally to the severity of the injury. Scientists have calculated and confirmed this proportionality in clinical settings, finding that in extreme cases the body may be reduced to less than half its original weight before recovery is achieved or, if the process cannot be halted, death occurs.
The Scientific Miracle — Wakefulness and Fever
With the physiological reality established, we return to the hadith. The Prophet ﷺ described the body’s response in two words: al-sahar (wakefulness) and al-humma (fever). Science has confirmed not only that both phenomena occur, but that they are independent, necessary, and ordered — wakefulness first, fever following it — precisely as stated.
Wakefulness (Al-Sahar)
Linguistically: insomnia, sleeplessness. Physiologically: a state of functional activity in the body’s vital systems that exceeds normal wakefulness — all organs remain continuously active and alert regardless of whether the patient appears consciously asleep or is even in a coma.
Common understanding assumes that wakefulness in illness is simply caused by pain. This is incorrect. Wakefulness is an independent, structured, and necessary process — not a secondary effect of discomfort. It is governed by a dedicated centre within the reticular formation that maintains continuous mutual stimulation between the hypothalamus, the reticular activation system, and the sympathetic nervous system, keeping every organ in functional alertness around the clock.

This wakefulness encompasses the entire body: the heart maintains its accelerated pumping, the kidneys their active filtration and potassium excretion, the liver its intensive metabolic activity, the immune system its heightened production of antibodies and defence cells — all through every hour of night and day. A patient in deep coma from severe head injury may appear completely unconscious, yet every other organ system remains in a state of extreme functional activity. The eyes close; the body never truly sleeps.
The reason is clear when we consider what sleep means for the body compared to wakefulness. Sleep is a state of reduced cardiac output, lowered metabolic rates, relaxed muscles, decreased respiratory depth, and falling body temperature — a general restoration mode in which every organ slows. To enter this state with a seriously injured organ requiring urgent emergency supply would be disastrous — like a town under attack at night deciding to postpone its defence until morning. Functional wakefulness is therefore not a symptom of illness; it is one of the body’s primary weapons against it.
Fever (Al-Humma)
Fever is not a sign of the disease overwhelming the body. It is a weapon produced by the body itself, deliberately and purposefully, as part of its coordinated response.
Substances released by white blood cells and injured tissue during immune activity — most importantlyinterleukin-1. Pyrogens travel through the bloodstream to the hypothalamic temperature-control centres, resetting the body’s temperature setpoint upward and triggering the fever response.
When phagocytic cells engage with bacteria or damaged tissue, pyrogens enter the bloodstream and reach the hypothalamus, causing it to register the normal 37°C as cold. The body responds by activating heat-acquisition mechanisms — shivering, skin vessel contraction, raised hair — until the temperature climbs to the new setpoint. This explains the characteristic chills and shivering that precede a fever: the body is generating heat because the hypothalamus believes it is cold.
Three benefits of fever have been scientifically established. Regarding metabolic acceleration:
Metabolic reaction rates increase by approximately 10% for every 1°C rise in body temperature above normal. Since illness demands accelerated metabolic activity across all organ systems, fever directly serves the body’s emergency energy requirements.
The second benefit addresses the microbial threat directly:
Most pathogenic bacteria reproduce optimally at temperatures slightly below the human body’s normal 37°C. A fever of 38–40°C impairs their rate of reproduction, reduces their metabolic activity, and may cause their decline and death — effectively besieging the invader within the body’s own tissues.
The third benefit concerns the delivery of oxygen to repair sites:
Elevated temperature adjusts the rate at which oxygen separates from haemoglobin in red blood cells, causing oxygen to be released more readily to tissues at lower gas pressure — increasing the oxygen supply to cells engaged in intensive repair and immune activity.
It should be noted that not all degrees of fever are beneficial: brain cells are adversely affected above 40°C, their function is disrupted above 42°C, and life becomes unsustainable above 44°C.
The Linguistic and Rhetorical Miracle
The hadith describes the body’s total response with a single Arabic verb: تَدَاعَى (tadā’ā). This word carries multiple simultaneous meanings in classical Arabic, and each maps precisely onto a different dimension of the physiological response.
Tadā’ā as mutual calling: the sensation centres call the hypothalamic control centres; those call the pituitary; the pituitary calls the endocrine glands; the endocrine glands call every organ to direct its functions toward the affected part. The complaint of a single injured organ sets off a cascade of calling between systems that spans the entire body.
Tadā’ā as gathering and converging from all directions: the simultaneous mobilisation of the circulatory, immune, hormonal, metabolic, and nervous systems toward a single point of injury — each arriving from its own axis, none waiting for the others.
Tadā’ā as collapse and demolition (as in walls crumbling to ruin): the body demolishes its own protein stores, fat reserves, and muscle mass in order to supply the injured organ with the energy and materials it needs. This demolition is real and measurable — scientists have confirmed it is proportional to injury severity, and that it continues even when patients are supplied with all necessary nutrition intravenously. All that medicine can achieve is to reduce its rate; it cannot be prevented. The body remains in this state of purposeful self-destruction until the complaint of the injured organ ceases.
Tadā’ā as preparing and mobilising for battle: the body entering a full emergency combat state — muscles tensed, heart accelerated, senses heightened, every resource redirected.
Every meaning of the single word tadā’ā describes a real and distinct phase of what happens in a living body during illness. No single alternative word in the Arabic language captures all four realities simultaneously.
Modern medicine calls the nervous system that activates in response to danger and disease the sympathetic nervous system. In English, “sympathetic” means compassionate — feeling with another, sharing in their distress. The Prophet ﷺ described the believers’ relationship to one another using the words tawādd (mutual love), taraḥum (mutual mercy), and taʿāṭuf (mutual compassion) — the same qualities. Scientists named the system for what it does biologically; the Prophet ﷺ named the same phenomenon fourteen centuries earlier in describing what believers owe one another morally.
The hadith also specifies the sequence: wakefulness and fever — wakefulness preceding, fever following. This is exactly what physiology has established: the neuroendocrine activation that constitutes systemic wakefulness is the first response, immediate upon injury; fever follows as a downstream product of immune cell activity, which is itself downstream of the initial neural alert cascade.
“And in yourselves — do you not see?”
Conclusion
- The injured organ genuinely complains — emitting nerve impulses, chemical signals, and hormones to the brain’s command centres through multiple simultaneous axes.
- The body genuinely responds (tadā’ā) — calling, converging, demolishing its own reserves, and mobilising for battle — directing every organ system toward the one site of injury.
- Wakefulness is a real, independent, systemic state, maintained in every organ continuously throughout illness — even during unconsciousness and coma — not a mere side effect of pain.
- Fever is a real, purposefully triggered weapon of the body, following wakefulness in precisely the order named, serving as metabolic accelerant, bacterial suppressor, and oxygen delivery enhancer simultaneously.
What those who preceded modern physiology understood only as eloquent metaphor, science has confirmed as literal biological description.
The hadith also carries a jurisprudential dimension: whoever wishes to understand the degree of love, mercy, and compassion the Prophet ﷺ demanded between believers should first ask medical experts how a single body responds to the injury of one of its parts — the total collapse of every other organ in service of the one that suffers. That is the standard set for the Muslim ummah.
“And Allah has sent down upon you the Book and wisdom and taught you that which you did not know. And ever has the favour of Allah upon you been great.”
References
- Council of Arab Health Ministers / World Health Organization — Unified Medical Dictionary (English–Arabic–French), 1983.
- Ibn Hajar al-Asqalani, Fath al-Bari — Sharh Sahih al-Bukhari, Vol. 10, p. 438, Hadith 6011 (Book of Literature), Imam Muhammad ibn Saud Islamic University, Riyadh.
- Imam al-Nawawi, Riyad al-Salihin, ed. al-Albani, Hadith No. 299, p. 131, Islamic Office, Beirut and Damascus.
- Ibn Manzur, Lisan al-Arab, Dar Sadir, Beirut.
- Guyton, A. (1984). Textbook of Medical Physiology, 6th ed. W.B. Saunders, Philadelphia.
- Ganong, W.F. (1989). Review of Medical Physiology. Appleton & Lange. pp. 537, 107, 301, 25, 280, 209–211, 266.
- Wall, P.D. & Melzack, R. (1989). Textbook of Pain. Churchill Livingstone, Edinburgh.
- Axelrod, J. & Reisine, T.D. (1984). Stress hormones: their interaction and regulation. Science, 224, 425.
- Williamschumer (1987). Homeostasis and shock. In: Sabiston, D.C., Essentials of Surgery, Ch. 2. W.B. Saunders, Philadelphia.
- Baue, A.E. & Chaudry, I.H. (1980). Prevention of multiple system failure. Surgical Clinics of North America, 60, 1167.
- Graham, I. Hill (1995). Nutrition in surgical practice. In: Cuschieri, Giles & Moosa, Essential Surgical Practice, 3rd ed. Butterworth-Heinemann.