The Recurrent Laryngeal Nerve — Is It Evidence of Poor Design? A Scientific Rebuttal
Response to the Recurrent Laryngeal Nerve Argument Against Intelligent Design
Table of Contents
- The Evolutionist Claim
- Preliminary Response — The Nerve Performs Its Function Perfectly
- Problem 1 — Indirect Paths Are Common and Functional
- Problem 2 — The Detour Serves Multiple Functional Purposes
- Problem 3 — The Direct Route Causes Pathology
- Problem 4 — Developmental Constraints, Not Evolutionary Heritage
- Conclusion — Developmental Constraints Serve the Larynx and Heart
- Recommended Reading
The Evolutionist Claim
They argue that an unnecessary detour of this kind can only be explained by evolutionary inheritance from fish ancestors.
Jerry Coyne, Why Evolution is True?, p. 88
Preliminary Response — The Nerve Performs Its Function Perfectly
The nerve essentially performs its function perfectly. Its functional value is fully achieved — and the achievement of that function negates any claim of unnecessary design. Merely imagining a different structure that could theoretically perform the same function does not detract from the basic functional value of the existing one.
Problem 1 — Indirect Paths Are Common and Functional
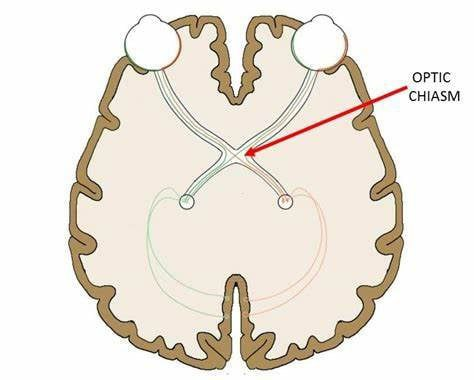
For example: the two optic nerves do not go directly to the occipital lobe of the brain. Instead, they intersect at the optic chiasm (in the shape of an X), following this path:
Retina → Optic nerve (2nd cranial nerve) → Optic chiasm → Optic tract → Lateral geniculate bodies + hypothalamus → Optic radiations → Visual cortex
This indirect route serves fundamental purposes: organizing visual information, improving vision, and adapting to injury.
See also: Ashley C. Ireland; Iverson B. Carter. Neuroanatomy, Optic Chiasm. PubMed, NIH.
Problem 2 — The Detour Serves Multiple Functional Purposes
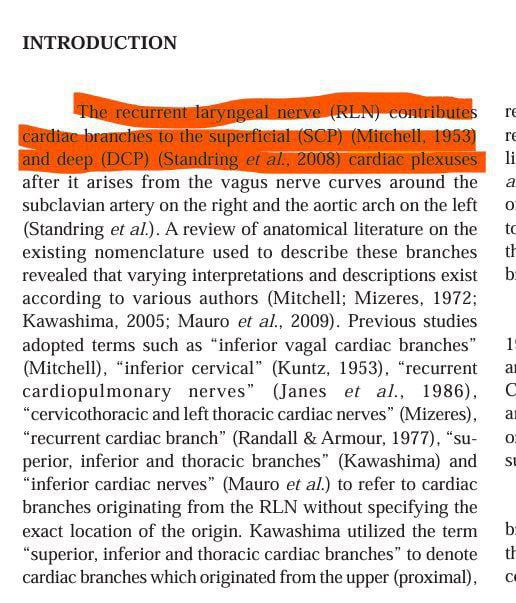
Cardiac Contributions
- The Superficial Cardiac Plexus (SCP)
- The Deep Cardiac Plexus (DCP)
The branch in question is specifically described as the recurrent laryngeal cardiac nerve — a cardiac branch arising directly from the recurrent laryngeal nerve, reaching the superficial or deep parts of the cardiac plexus.
- Standring, S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 40th ed. Edinburgh, Churchill Livingstone/Elsevier, pp. 459, 588–589.
- Mitchell GA. The Innervation of the Heart. Br Heart J. 1953 Apr;15(2):159-71. doi: 10.1136/hrt.15.2.159. PMID: 13041995; PMCID: PMC479482. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC479482/
https://www.researchgate.net/publication/263859400_The_Recurrent_Laryngeal_Cardiac_Nerve_in_Fetuses
Branches Supplied During Ascent
- The mucous membrane of the muscular covering of the esophagus
- The muscle fibers of the trachea
- The inferior pharyngeal sphincter

Sturniolo G, D’Alia C, Tonante A, Gagliano E, Taranto F, Lo Schiavo MG. The recurrent laryngeal nerve related to thyroid surgery. Am J Surg. 1999 Jun;177(6):485-8. doi: 10.1016/s0002-9610(99)00101-4. PMID: 10414699.
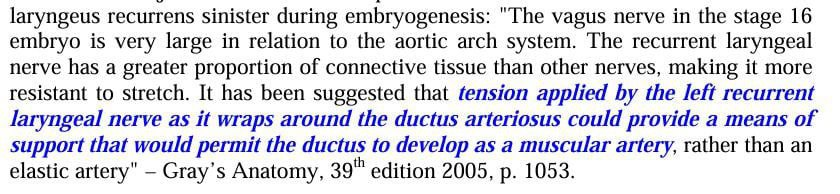
Embryonic Function — The Ductus Arteriosus
Problem 3 — The Direct Route Causes Pathology
This is a pathological condition, not an improvement.
Armstrong WG, Hinton JW. Multiple divisions of the recurrent laryngeal nerve. An anatomic study. AMA Arch Surg. 1951 Apr;62(4):532-9. DOI: 10.1001/archsurg.1951.01250030540011. PMID: 14810348.
Problem 4 — Developmental Constraints, Not Evolutionary Heritage
How Embryogenesis Explains the Detour
Blechschmidt, E. 2004. The Ontogenetic Basis of Human Anatomy: A Biodynamic Approach to Development from Conception to Birth. B. Freeman, transl. New York: North Atlantic Books, p. 188.
- The precision involved in embryogenesis
- The risks posed by even the smallest developmental change
- The irreducible complexity of the mechanical synchronization of organs
Various arteries and structures must be elongated, and organs must move in such a way that they maintain their function throughout this developmental stage.
Sadler, T.W. 1990. Langman’s Medical Embryology, 6th ed. Philadelphia, PA: Williams & Wilkins, p. 211.
Schoenwolf, G.C., S.B. Bleyl, P.R. Brauer, and P.H. Francis-West. 2009. Larsen’s Human Embryology. Philadelphia, PA: Churchill Livingstone, p. 407.
The course of the recurrent laryngeal nerves then becomes different on the right and left sides due to the downward movement of the heart.
Sadler, 1990, Langman’s Medical Embryology, p. 211.
The Phrenic Nerve — A Parallel Case
This is a necessary pathway because the pericardium and diaphragm originate in the transverse septum — a thick mass of tissue from which parts of the thoracic diaphragm and the ventral mesentery of the foregut arise — in the neck region of the early fetus. The structure then migrates as the fetus grows through differential growth of the head and thoracic regions, taking the nerve with it.
The diaphragm cannot develop in stages — because a partial diaphragm results in an incomplete separation of the thorax and abdomen. Any slight defect could cause intestinal contents to herniate into the chest, compressing the lungs or causing intestinal strangulation.
The Ligamentum Arteriosus as a Pulley
The body must function as a living, functional unit during this time — requiring ligaments and internal connections to secure the various related structures together while also allowing movement of the body and organs.
For the laryngeal nerve, the ligamentum arteriosus acts like a pulley — lifting a heavy load to allow movement.
During this phase, the reducibility of all systems is zero — all of this movement, its functional integration, and the requirement for synchronization are the critical factors that allow the downward movement of the left recurrent laryngeal nerve.
Blechschmidt, The Ontogenetic Basis of Human Anatomy, p. 91.
Conclusion — Developmental Constraints Serve the Larynx and Heart
- Functional necessity — the nerve contributes to the cardiac plexuses, esophagus, trachea, and inferior pharyngeal sphincter along its path
- Embryonic precision — its wrap around the ductus arteriosus supports the development of that vessel as a muscular rather than elastic artery
- Developmental constraint — the path is determined by the mechanics of embryogenesis, not evolutionary inheritance
- The direct route is pathological — it corresponds to the real medical condition NRLN, which is associated with vascular abnormality
Developmental constraints and functional purposes are both evident from the anatomy. The sending of branches to the cardiac plexus and other organs leads us unambiguously to conclude that these constraints serve the larynx and the heart — not any alleged evolutionary heritage.
Recommended Reading
📚 The Evolution of the Long-Necked Giraffe (Giraffa Camelopardalis L.) Verlagshaus Monsenstein & Vannerdat oHG, 2011.
This work encompasses the details of the subject and presents an impressive review combining two previous works. Its strength lies not only in responding to and refuting the arguments of evolutionists, but also in presenting problems from within their own framework — turning the argument against them on their own terms.
This article is part of the OpenIslam Wiki — Responses to Evolutionary and Materialist Arguments series.